
How we imagine the future of the profession. Between fear and potential.
The debate about artificial intelligence in psychotherapy is most often conducted within two extreme frames. The first is fear: a picture in which an algorithm takes over the profession, and therapeutic competencies - the relationship, years of training, clinical reasoning - are reduced to a footnote. The second is uncritical enthusiasm: the assumption that a tool will solve problems that until now required a human being. Both frames oversimplify what a therapist’s work really is. The graphic opening this article places them side by side on purpose.
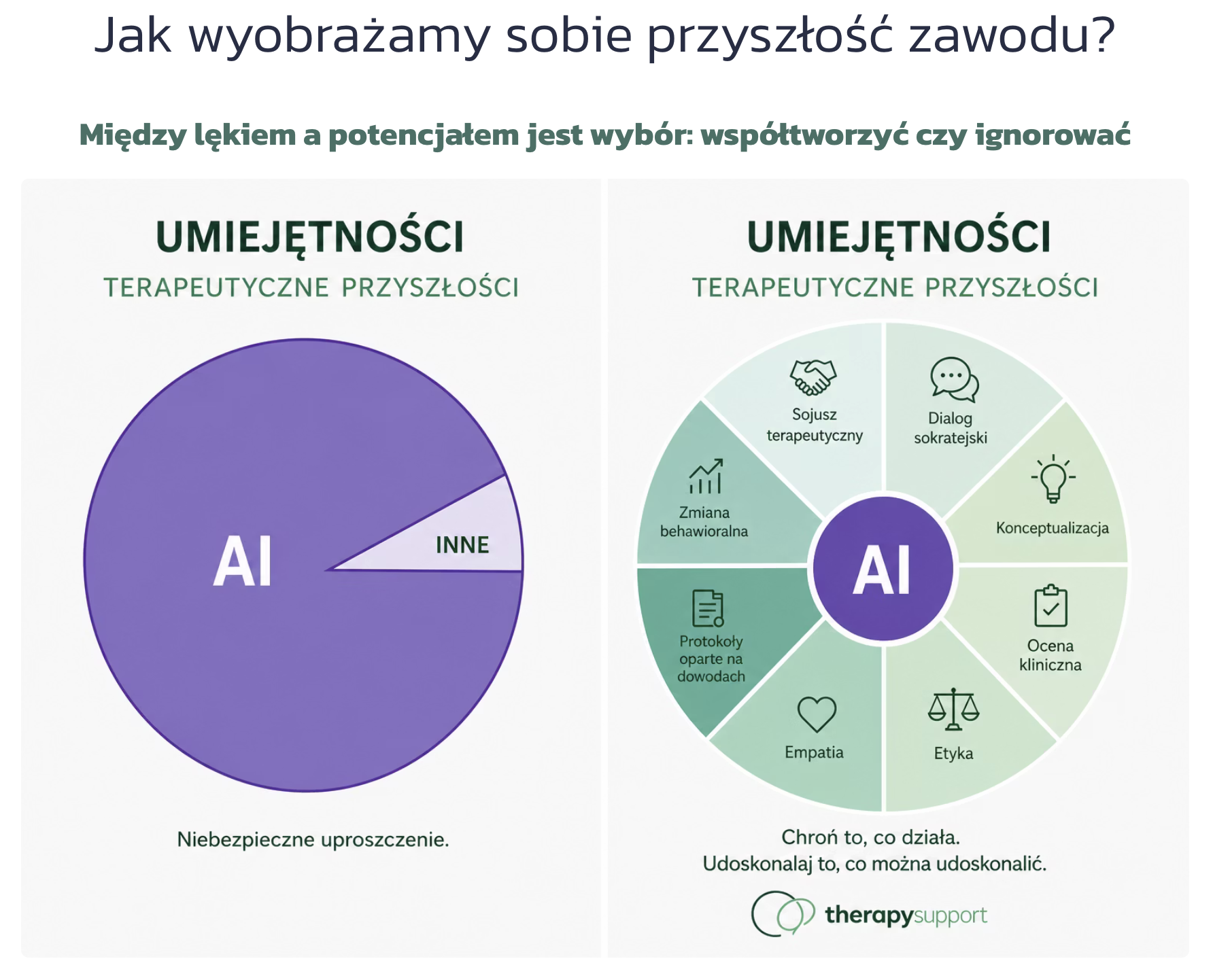
The left side: a dangerous oversimplification
The first diagram presents the “therapeutic skills of the future” as a near-uniform field of AI, with a residual “other” category. It is a vision in which technology takes the place of competence instead of supporting it. It is convenient, because it lets you either reject AI entirely or trust it without limit - in both cases without having to draw any boundaries. And that is exactly why it is misleading.
The right side: AI around competencies, not instead of them
The second diagram organises those same future skills according to what they are in clinical practice: the therapeutic alliance, Socratic dialogue, case conceptualisation, clinical assessment, ethics, empathy, behavioural change, and evidence-based work. AI sits at the centre not as a decision-making agent, but as a supporting layer - relieving the therapist of documentation and of organising material, in order to free up time for what remains uniquely human. None of the eight competencies is a subject of automation.
This distinction has an empirical basis
Two large randomised trials from 2026 show the same pattern. McFadyen and colleagues (Communications Medicine), in a study of 540 people, found that a CBT app supported by generative AI was used more often and for longer than the digital control material, with comparable clinical effectiveness. So and colleagues (Journal of Medical Internet Research), in a three-arm trial of 1,187 people, observed no significant differences in the reduction of depressive symptoms (PHQ-9), but did record higher engagement in the AI-supported group.
The conclusion is consistent: AI-supported tools increase patient engagement, but the clinical outcome remains comparable to the control group. Engagement is a predictor of effect, not the effect itself.
The most interesting finding, however, concerns what drives patient retention in therapy. In So and colleagues’ exploratory analysis, retention was driven by the model’s empathic function - the reflection of emotion - with an odds ratio close to ten (OR 9.99), whereas the advisory function showed no significant effect. The mechanism is therefore not “giving accurate advice”, but reflecting emotion. And that is a competency whose core remains with the therapist.
A boundary that must be drawn deliberately
Ignoring the change will not stop it - it will only ensure that it happens without the people who best understand what safe, ethical, relationship-based therapy is. The answer is not to give up the technology, but to choose tools whose compliance is documented rather than merely declared.
In that sense the principle written on the graphic - protect what works; improve what can be improved - is not a marketing slogan but an operational criterion. Between fear and potential there is a choice: to co-create or to ignore.
Protect what works. Improve what can be improved.
This text analyses published scientific data and does not constitute a clinical recommendation. Therapy Support is not a medical device within the meaning of the MDR and does not make clinical decisions. AI in the platform supports documentation and the organisation of material - all clinical decisions remain with the therapist.
Sources: J. McFadyen et al., Increasing engagement with cognitive-behavioral therapy (CBT) using generative AI: a randomized controlled trial (RCT), Communications Medicine 6, 129 (2026), nature.com/articles/s43856-025-01321-8. M. So et al., Effect of AI-Based Natural Language Feedback on Engagement and Clinical Outcomes in Fully Self-Guided Internet-Based Cognitive Behavioral Therapy for Depression: 3-Arm Randomized Controlled Trial, Journal of Medical Internet Research (2026), jmir.org/2026/1/e76902.